The following is Chapter Two from the book Loving Variant Minds: How to Navigate Love After a Late Neurodivergence Diagnosis.
Available on Apple Books, Kindle and paperback.
Chapter 2: ADHD Explained
What is ADHD?
Chances are that if you are reading this book, ADHD is the factor that brought you here. With ADHD affecting an estimated five to seven percent of the population 12, and around half of those with autism also meeting criteria for ADHD 345, understanding what this condition actually is becomes a critical element of learning to live with it - whether you have it yourself or love someone who does.
But what is ADHD? The answer depends on who you ask, and more importantly, on what level of complexity you are ready to engage with. I have found that much of the confusion and frustration surrounding ADHD stems from people talking past each other - operating at different levels of understanding without realising it. So before diving into the neuroscience, let me walk you through how understanding of ADHD typically develops, from the simplest explanations to the most nuanced.
Most people first encounter ADHD through specific individuals. “My nephew has ADHD - he’s the one who can’t sit still at family dinners.” “There was a kid in my class who had ADHD; he was always in trouble.” “Isn’t that what that celebrity said they have?” At this stage, there is no real concept of what ADHD is as such - just a collection of examples we try to piece together into a pattern. The problem is that every person with ADHD presents differently, so these concrete examples can be misleading. If your only reference point is a hyperactive ten-year-old boy, you might not recognise ADHD in a quietly struggling adult who has learned to mask their difficulties.
As understanding develops a little further, ADHD becomes a category - something you either have or you do not. At this level, the condition tends to be characterised as either fundamentally good or fundamentally bad. You will hear people say “ADHD is a superpower” or “people with ADHD are so creative” on one side, and “ADHD is a serious disorder” or “it ruins lives” on the other. There is little room for the reality that it can be both, depending on context and support. This level of thinking also produces ideas like “mild” versus “severe” ADHD, and the dismissive “everyone’s a little bit ADHD.” These statements are not entirely wrong, but they flatten something complex into something overly simple.
A more sophisticated understanding recognises ADHD as neurodevelopmental - a condition rooted in how the brain develops. At this level, we can hold complexity: someone can be both gifted and impaired, can have extraordinary strengths in some areas and significant gaps in others. ADHD is no longer one single difference but a profile of differences across multiple domains - attention regulation, impulse control, emotional management, time perception, working memory - that combine uniquely in each person. This is the level at which clinical diagnosis and most medical treatment operates.
The most complete understanding zooms out further still to consider the systems within which individuals exist. Here, we recognise that neurological differences like ADHD are natural variations in human brain development - present throughout human history and not inherently pathological. We see that much of what “disables” someone with ADHD is not the brain difference itself but environments, expectations, and systems designed without neurodivergent people in mind. Schools demand sustained attention on unstimulating material. Workplaces assume reliable executive function. Social norms expect consistent emotional regulation. When these environments clash with how the ADHD brain operates, the result is impairment - but the impairment emerges from the mismatch, not solely from the individual.
I share this progression because you will encounter all of these levels of understanding as you navigate life with ADHD in the picture. Your doctor may operate at the clinical level, focusing on symptoms and treatment. Your family members may be stuck at the level of concrete examples, comparing you or your partner to the one person with ADHD they have known. Online communities may swing between “ADHD is a gift” and “ADHD has destroyed my life.” Recognising where someone’s understanding sits can save you enormous frustration - and help you meet them where they are rather than talking past each other.
For the purposes of this book, I will primarily work at the more developed levels of understanding. ADHD is a neurodevelopmental condition, meaning it originates in how the brain grows and matures, shaped by genetics and neurology rather than by parenting, trauma, or personal choices. It represents a genuine developmental difference - not a character flaw, not a moral failing, not the result of too much screen time or poor discipline.
More specifically, ADHD involves delays in the biological development of certain brain functions, particularly those governing self-regulation, attention management, and impulse control. Dr Russell Barkley, one of the world’s leading ADHD researchers, describes it as a delay in two key dimensions: executive functioning (often mislabelled as “inattention”) and behavioural inhibition (the hyperactivity and impulsivity symptoms) 6. The brain regions responsible for these functions develop on a different timeline - running approximately two to three years behind neurotypical peers in childhood, with this gap persisting in various forms into adulthood 7.
The word “delay” matters here. ADHD is not a qualitative difference - the ADHD brain does not work in a fundamentally alien way. It is a quantitative difference, measurable in brain imaging studies and observable in behaviour. This framing shifts us away from moral judgment. When someone with ADHD forgets an important appointment, loses their keys for the third time this week, or interrupts you mid-sentence, they are not being careless, disrespectful, or lazy. Their brain is operating with a genuine developmental difference in the very systems responsible for these functions.
At the same time, ADHD can be substantially disabling, particularly when undiagnosed or untreated. While many of its challenges can be mitigated through ongoing management and environmental adaptation, the underlying vulnerabilities remain. The extent of impairment often reflects the degree of support, recognition, and structure available rather than the severity of the condition itself. An ADHD brain in a stimulating, flexible environment with appropriate support may flourish. The same brain in a rigid, understimulating environment - constantly demanded to sustain attention on unengaging tasks - may struggle enormously. The difficulty is not located solely within the individual; it emerges from the interaction between the individual and their environment. This understanding does not excuse harmful behaviour or absolve anyone of responsibility. But it does change how we approach problems - moving from “why can’t you just try harder?” to “what support and structures would actually help?”
ADHD is highly heritable. Research consistently shows that if you have ADHD, there is roughly a 40% chance that any children you have will also have it 8. For decades, ADHD was considered a childhood condition that people “grew out of.” We now know this to be incorrect. While hyperactivity symptoms often diminish with age, the core difficulties with executive function, attention regulation, and impulse control persist into adulthood for at least 60–70% of those diagnosed in childhood 9. It is important to understand what this figure actually reflects. It describes who continues to meet the formal diagnostic criteria as adults, not who continues to have ADHD. Many individuals fall below the diagnostic threshold not because the underlying traits have vanished, but because they have learned to cope, to compensate, or simply to mask their difficulties.
This same dynamic operates in the opposite direction as well. Many children with quieter or more internalised ADHD presentations were never identified in the first place. Their struggles were dismissed as personality quirks, lack of effort, or “daydreaming”, and their genuine neurodevelopmental differences went unrecognised. These are the people who often reach their thirties, forties, or fifties before encountering a description of ADHD that finally makes sense of their lifelong patterns.
In this respect, ADHD is best understood as a lifelong condition whose visibility changes over time. Symptoms shift, environments shift, and people adapt, but the underlying profile remains.
Throughout this chapter, I will explain what is happening in the ADHD brain, how this manifests in daily life, and why understanding the neurobiology can help reduce shame and improve relationships. We will look at the role of dopamine, examine brain imaging research that shows measurable differences, explore the often-overlooked role of emotional regulation, and address conditions that frequently accompany ADHD. My aim is to give you a foundation of understanding that will serve you throughout this book and, more importantly, throughout your life and relationships.
The Dopamine System: Understanding the Brain Chemistry
To understand ADHD, we need to understand dopamine. You have probably heard of dopamine described as the brain’s “pleasure chemical” or “reward molecule.” This is not quite accurate. Dopamine is better understood as a chemical messenger involved in motivation, reward anticipation, and learning. It does not create happiness so much as it creates wanting - the drive to pursue things that matter to us 10.
Dopamine is a neurotransmitter, one of the chemical messengers that allow brain cells (neurons) to communicate with each other. The process works like this: dopamine is manufactured inside neurons from an amino acid called tyrosine. Once produced, it is packaged into tiny storage containers called vesicles. When a neuron fires, these vesicles release dopamine into the gap between neurons - the synaptic cleft - where it can bind to receptors on the neighbouring neuron and transmit its signal. Put simply, a neuron operates electrically within the cell, but it communicates chemically with other neurons using neurotransmitters, of which dopamine is one of the principal examples. After the message is delivered, dopamine is either broken down by enzymes or recycled back into the original neuron through a process called reuptake 11.
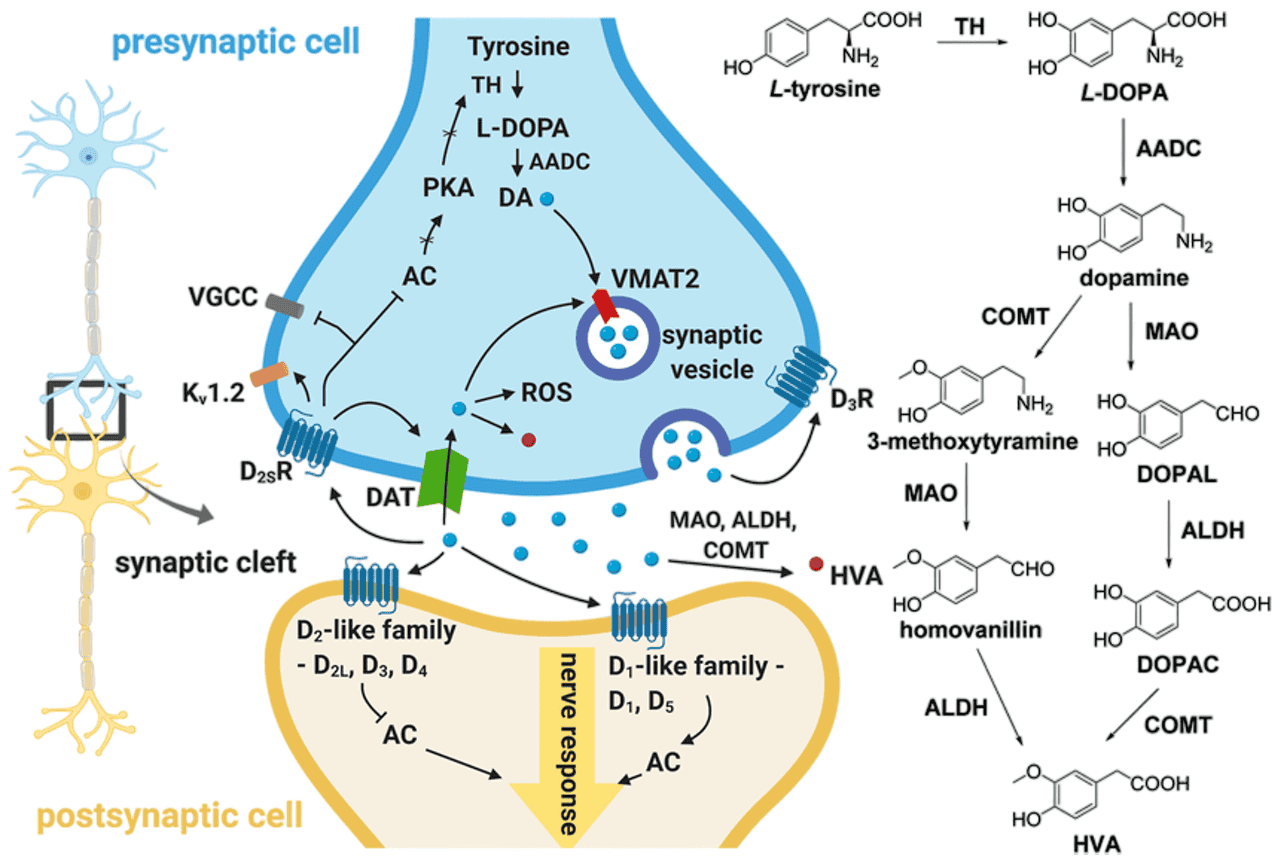
Figure 1 12
Dopamine is produced by specialised neurons located mainly in the midbrain, particularly the substantia nigra and the ventral tegmental area. These neurons send long projections throughout the brain, forming four major dopaminergic pathways, each responsible for different aspects of movement, motivation, cognition, and hormonal regulation:
The Nigrostriatal Pathway runs from an area called the substantia nigra to the striatum. This pathway is primarily involved in movement and motor control. When this pathway degenerates, the result is Parkinson’s disease, characterised by tremors and difficulty initiating movement.
The Mesolimbic Pathway connects the ventral tegmental area to the nucleus accumbens and amygdala. This is the pathway most associated with reward, motivation, and emotion. It drives pleasure-seeking behaviours and is heavily implicated in addiction.
The Mesocortical Pathway also originates in the ventral tegmental area but projects to the frontal cortex. This pathway is crucial for cognition, attention, memory, and decision-making - the very functions most affected in ADHD.
The Tuberoinfundibular Pathway runs from the hypothalamus to the pituitary gland and is involved in hormone regulation, particularly the inhibition of prolactin.
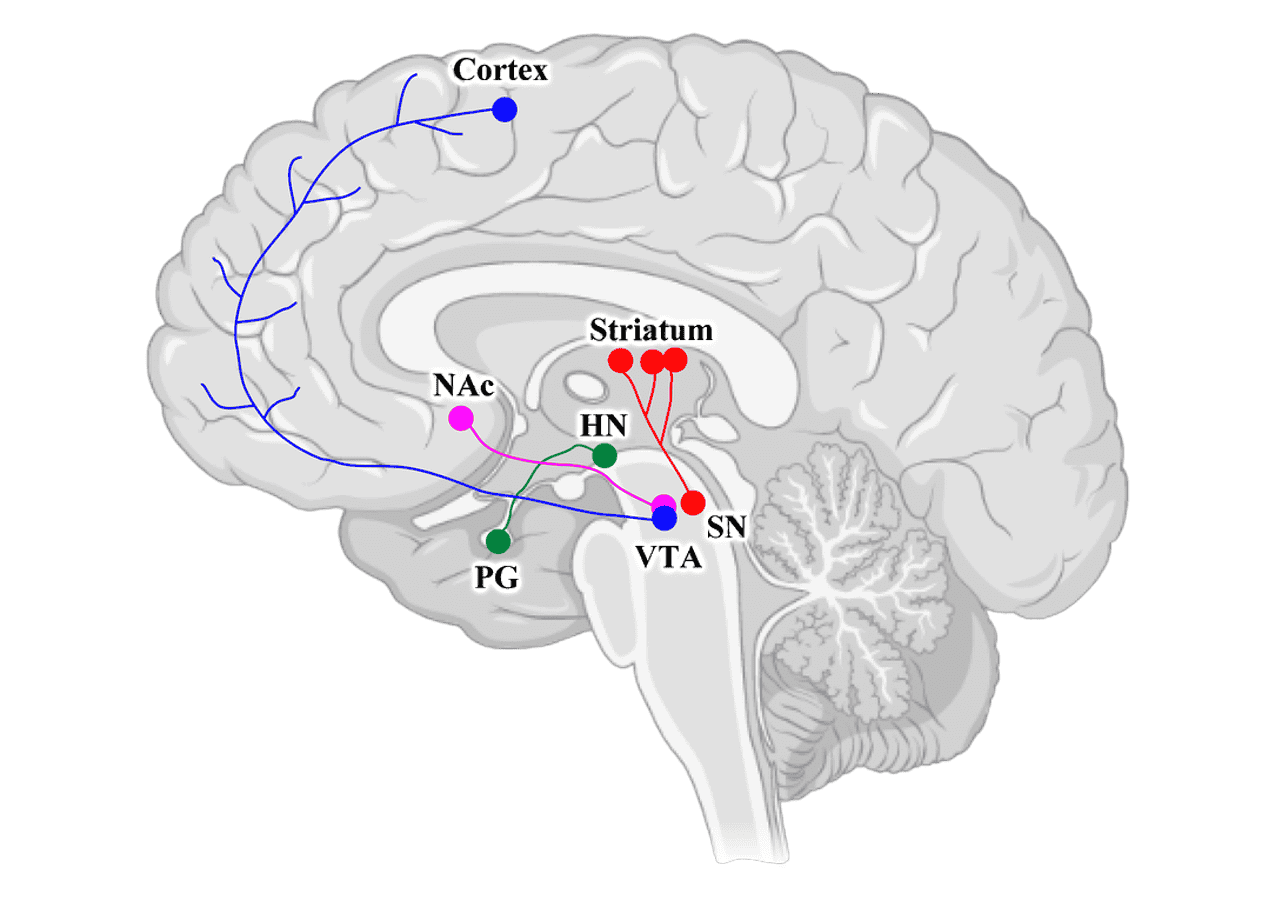
Figure 2 13
In ADHD, the problem is not that there is too little dopamine in the brain overall. Rather, the issue lies in how dopamine is regulated and utilised, particularly in the mesocortical and mesolimbic pathways. One influential theory highlights differences in dopamine transporter density, the proteins responsible for recycling dopamine back into neurons. In some individuals, dopamine may be cleared from the synaptic cleft too quickly, reducing its functional availability 14.
Other research points to additional mechanisms, including differences in dopamine production, vesicular storage, or receptor sensitivity in the prefrontal cortex. These findings vary between studies, and the modern understanding is that ADHD reflects a broader dysregulation of dopaminergic signalling rather than a simple deficiency or excess 815. The exact pattern differs across individuals, but the end result is the same: the circuits responsible for attention, motivation, and executive control do not receive dopamine in the way they need.
These differing mechanisms also help explain why there are several classes of ADHD medication, each acting on dopamine and noradrenaline systems in slightly different ways. Because ADHD does not arise from a single neurochemical pattern, no clinician can determine in advance which medication will be the best fit for a particular individual. The initial prescribing process is therefore inherently exploratory. Psychiatrists start with a reasonable first option, then rely heavily on the patient’s own experience of focus, emotional stability, side effects, and daily functioning to refine the dosage or switch to an alternative. This trial-and-response approach is not a sign of uncertainty or poor practice, but simply a reflection of the underlying neurobiological variability within ADHD.
Regardless of the theory, the result is the same - a brain that struggles to maintain consistent activation in the frontal regions responsible for attention, planning, and impulse control. This is why stimulant medications - which increase dopamine availability in the synapse - are so effective for many people with ADHD. They are not giving the brain something foreign; they are helping the brain’s natural systems work more effectively.
To understand how this works, it helps to know what “reuptake inhibitor” means - a term you will encounter frequently if you explore ADHD medication. After dopamine is released into the synaptic cleft and delivers its signal, the sending neuron does not simply leave it there. It consumes the dopamine back up through specialised proteins called transporters - this recycling process is reuptake. In ADHD, this reuptake may happen too efficiently, clearing dopamine from the synapse before it has had adequate time to do its job.
Most ADHD medications work by blocking or slowing this reuptake process. Methylphenidate (sold under brand names like Ritalin and Concerta) and amphetamine-based medications (such as Adderall and Vyvanse) both increase dopamine availability in the synapse, though through slightly different mechanisms. By preventing the dopamine transporter from clearing dopamine so quickly, these medications allow dopamine to remain in the synaptic cleft longer, giving it more opportunity to bind to receptors and transmit its signal effectively.
This is why stimulant medications, counterintuitively, often have a calming effect on people with ADHD. The ADHD brain is not under-stimulated in a general sense, but rather unevenly stimulated. Some circuits, especially those involved in reward and emotional reactivity, can become overwhelmed, while the frontal regions responsible for planning, attention, and inhibition remain underactivated. This imbalance drives the familiar restlessness and constant search for stimulation, because the brain is attempting to compensate for low baseline activation where it matters most.
Stimulant medication increases dopamine availability across these networks, which reduces the brain’s need to chase stimulation and allows the prefrontal systems to reach a more functional level of activation. In neurotypical individuals, this same increase would push dopamine levels above the optimal range and feel overstimulating. In ADHD, it brings the system closer to balance, which is why stimulants often make people with ADHD feel calmer, more focused, and more settled.
It is worth pausing here to address a common misconception. Dopamine is often called the “happiness chemical,” but neuroscience research has consistently shown that dopamine is more about wanting than liking. It creates the motivation to pursue rewards, not the pleasure of receiving them. Actual pleasure involves other neurotransmitter systems, including endorphins and endocannabinoids 16. This distinction matters because it helps explain some of the behaviours we see in ADHD: the restless pursuit of stimulation, the difficulty sitting with boredom, the tendency to chase novelty. The ADHD brain is not pleasure-seeking in a hedonistic sense - it is stimulation-seeking in a way that reflects its neurochemical reality.
Understanding this also helps explain why people with ADHD often self-medicate, whether consciously or unconsciously. Nicotine, caffeine, and even high-risk behaviours can temporarily boost dopamine signalling, providing relief from the chronic understimulation that characterises the ADHD experience. This is not moral weakness - it is neurobiology driving behaviour. We’ll be expanding on these tendencies later in Chapter 7.
Seeing the Difference: Brain Imaging Evidence
For many years, ADHD diagnosis relied entirely on behavioural observation and self-report. There was no blood test, no scan, no objective marker that could confirm the condition. This led some to question whether ADHD was “real” or merely an excuse for poor behaviour. Brain imaging research has fundamentally changed this picture.
Dr Daniel Amen and his colleagues have conducted extensive research using SPECT (Single Photon Emission Computed Tomography) imaging to examine blood flow and activity patterns in the brains of people with ADHD. SPECT scans measure regional cerebral blood flow, which serves as a proxy for brain activity - areas with more blood flow are more active.
In a significant study comparing over 1,000 ADHD patients to healthy controls, Amen’s team found consistent patterns of difference. The ADHD group showed significantly lower activity in several key regions, particularly the prefrontal cortex - the area responsible for executive functions like planning, decision-making, and impulse control. Specifically, decreased perfusion was observed in the orbitofrontal cortices, anterior cingulate gyri, areas of the prefrontal cortices, basal ganglia, and temporal lobes 17.
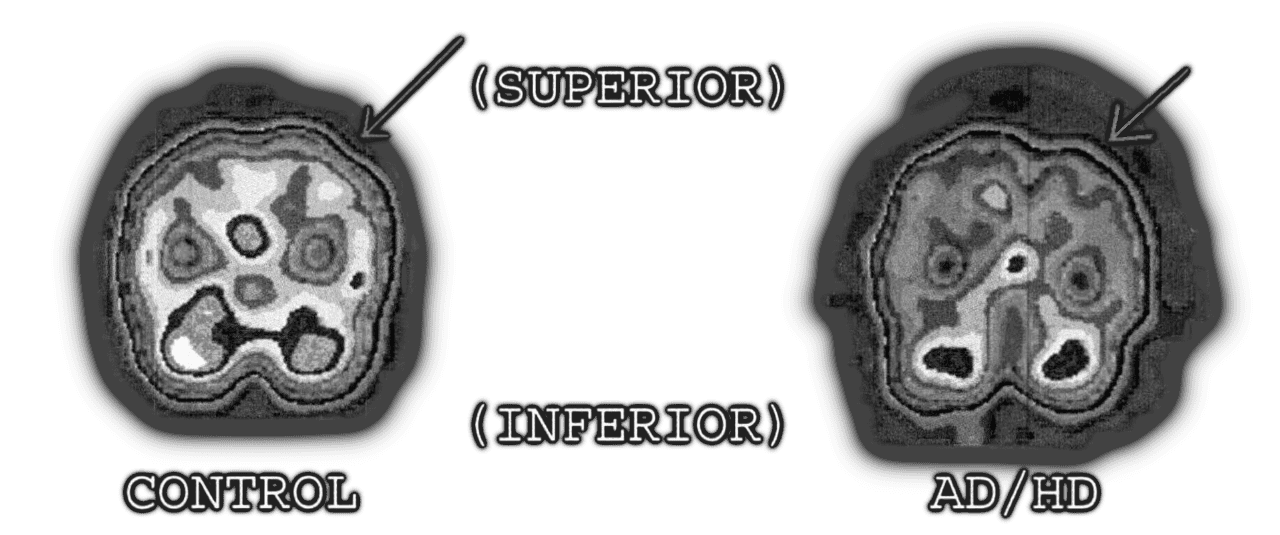
Figure 3 18
What makes these findings particularly compelling is what happens during concentration tasks. In neurotypical brains, when you focus on a demanding task, activity in the prefrontal cortex increases, so the brain “turns on” the regions needed for concentration. In many ADHD brains, the opposite occurs. When faced with a concentration task, prefrontal activity actually decreases. The very act of trying to focus seems to deactivate the regions required for focusing.
This paradoxical response helps explain why “trying harder” does not work for people with ADHD. When a neurotypical person needs to concentrate, they can recruit additional cognitive resources through effort. When someone with ADHD attempts the same thing, their brain may instead become less active in the crucial regions.
This feels counterintuitive. You would expect dopamine to be redirected to where it is needed and, at times, this can create the impression of intense focus. But this does not mean the underlying regulation is working well. Neuroimaging studies show that when someone with ADHD exerts effort to focus, the prefrontal cortex may paradoxically become less active, not more. One interpretation is that the brain is attempting to compensate for limited dopaminergic signalling, but because the baseline regulation is insufficient, this effort cannot be sustained. The result is reduced activation in the very circuits required for attention. This is why effortful concentration can feel both exhausting and ineffective for people with ADHD: the brain is working hard, but there simply is insufficient neurochemical support to sustain it.
This is not laziness or lack of effort. It is a neurobiological phenomenon that shows up on brain scans.
The imaging research also helps explain why stimulant medications work. Earlier SPECT studies showed that stimulant medication can correct low prefrontal activity, bringing blood flow in these regions closer to typical levels 19. The medication is not sedating the brain; it is activating underactive regions.
This research has also identified structural differences in ADHD brains. The brain regions involved in ADHD - the orbital frontal cortex, anterior cingulate, basal ganglia, and cerebellum - tend to be 3–10% smaller in volume and show developmental delays of approximately two to three years compared to neurotypical brains of the same age 7. These are not subtle differences visible only with sophisticated analysis; they are measurable, replicable findings that establish ADHD as a genuine neurobiological condition.
It is important to note that brain imaging is not currently used for routine ADHD diagnosis - the research is still developing, and there is significant individual variation. However, these studies provide powerful validation for those who have spent their lives being told their struggles are not real or that they just need to “try harder.”
Core Features: Inattention, Hyperactivity, and Impulsivity
The diagnostic criteria for ADHD are organised around three core features: inattention, hyperactivity, and impulsivity. These can present in different combinations, leading to three recognised presentations: predominantly inattentive, predominantly hyperactive-impulsive, or combined presentation. Understanding what these actually look like in daily life - beyond the clinical language - is essential.
Inattention
Inattention in ADHD is not about an inability to pay attention. People with ADHD can focus intensely on things that interest them, sometimes to the exclusion of everything else. The difficulty lies in directing and sustaining attention on tasks that are not inherently engaging. Dr Barkley argues that “inattention” is actually a misnomer for what are really problems with persistence, resistance to distraction, and working memory.
In practical terms, inattention might look like: starting multiple projects and finishing none of them; losing track of conversations mid-sentence; forgetting appointments despite having written them down; making careless errors in work not because of incompetence but because attention drifted at a crucial moment; spending hours on an engrossing task while urgent responsibilities go neglected.
Hyperactivity
Hyperactivity is often what people picture when they think of ADHD - the child bouncing off walls, unable to sit still. In adults, hyperactivity typically becomes less visible but does not disappear. It often manifests as internal restlessness, a constant feeling of needing to be doing something. Adults with ADHD might fidget, tap their feet, or feel uncomfortable in situations requiring them to sit quietly for extended periods. Some describe it as having a motor running inside them that never quite turns off.
Impulsivity
Impulsivity involves acting without adequate forethought about consequences. This can manifest in many ways: interrupting others in conversation, making snap decisions that are later regretted, difficulty waiting one’s turn, blurting out inappropriate comments, or making impulsive purchases. Impulsivity is not limited to behaviour - it extends to cognition and emotion. People with ADHD often make rapid decisions without fully considering the implications, which can lead to patterns of choices that seem bewildering to outside observers.
These three features combine differently in different people. Someone with predominantly inattentive presentation might be quiet, dreamy, and easily overlooked - their struggles are internal rather than disruptive. Someone with predominantly hyperactive-impulsive presentation might be energetic, talkative, and quick to act but have fewer difficulties with focus. Many people have the combined presentation, experiencing significant symptoms across all three domains.
It is also worth noting what these symptoms are not. They are not occasional lapses that everyone experiences. The diagnostic criteria require that symptoms be persistent, present across multiple settings (not just at work or just at home), and causing significant impairment. Everyone loses their keys sometimes; people with ADHD lose their keys with a frequency and consistency that materially disrupts their lives.
Executive Function: The Brain’s Control Tower
If you have ever wondered why someone with ADHD can spend six hours absorbed in a video game but cannot spend twenty minutes paying bills, the answer lies in executive function. Executive functions are the higher-order cognitive processes that allow us to plan, organise, initiate action, monitor our behaviour, and adjust our approach when things are not working. They are what allow us to work toward goals, resist temptations, and navigate the complexities of adult life. Executive function has been identified as being processed in the frontal lobe of the brain, that is directly fed dopamine from the mesolimbic and mesocortcal pathways - tying back to the dopamine pathways mentioned earlier. Dysfunction in these pathways thus has direct effect on the function of this brain region.
Dr Barkley has argued that ADHD is, at its core, a disorder of executive function - or as he puts it, “Executive Function Deficit Disorder” would be a more accurate name than ADHD. The seven major executive functions that ADHD disrupts include:
Self-awareness – the ability to monitor your own behaviour and mental state. People with ADHD often have reduced awareness of how their actions affect others or how much time is passing.
Inhibition – the ability to stop yourself from acting on impulse. This is often the most visible deficit, manifesting as interrupting, blurting out, or acting without thinking.
Non-verbal working memory – holding visual and spatial information in mind. This affects the ability to remember where you put things, visualise future events, or mentally manipulate images.
Verbal working memory – the internal voice that helps us think through problems, give ourselves instructions, and remember verbal information.
Emotional self-regulation – the ability to manage emotional responses, which we will discuss in detail shortly.
Self-motivation – the capacity to motivate yourself to complete tasks without external pressure or immediate rewards.
Planning and problem-solving – the ability to break down goals into steps, anticipate obstacles, and adjust strategies.
When these systems are impaired, the result is not stupidity or laziness - it is a profound difficulty with the mundane mechanics of adult life. Filing taxes requires initiating an unpleasant task, maintaining focus through boring paperwork, holding multiple pieces of information in working memory, resisting the temptation to do something more interesting, and planning the steps to completion. Each of these steps requires executive function. For someone with ADHD, each step is a potential point of failure.
This is why “just do it” advice is so unhelpful and often harmful. It assumes that the gap between intention and action is a matter of willpower. For people with ADHD, that gap is a neurological chasm. Understanding this changes how we approach support - both self-support and supporting a partner with ADHD. The goal is not to generate more willpower but to build external structures and systems that compensate for unreliable internal executive control. We will explore these strategies in later chapters.
The Missing Criterion: Emotional Dysregulation
If you or someone you love has ADHD, you have probably noticed that emotions can run hot. Frustration boils over quickly. Excitement becomes overwhelming. Disappointments feel catastrophic. Moods shift rapidly and intensely. Yet if you look at the official diagnostic criteria for ADHD, you will find almost nothing about emotional regulation. This is one of the most significant gaps between clinical criteria and lived experience.
Dr Russell Barkley has spent years arguing that emotional dysregulation should be considered a core feature of ADHD, not a secondary complication. The historical record supports him. For the first 170 years after ADHD-like conditions were first described, emotional difficulties were consistently included in clinical descriptions. Early accounts mentioned “passion,” “quickness to anger,” “inability to regulate affect,” and being “easily frustrated.” It was only when the American Psychiatric Association standardised diagnostic criteria in the 1960s and 1970s that emotional symptoms were dropped - likely because they were harder to measure reliably than behaviours like hyperactivity 6.
The neuroanatomical evidence strongly supports including emotion. The brain regions implicated in ADHD - particularly the orbital frontal cortex and anterior cingulate - are the same regions responsible for emotional regulation. These areas form what Barkley calls the “hot executive circuit,” linking the frontal lobes to the amygdala and limbic system. If these regions are developing on a delayed schedule, as brain imaging confirms, then emotional regulation problems are an inevitable consequence, not an optional extra.
Research confirms this. Studies consistently show that people with ADHD have significant difficulties with emotional regulation - not different emotions, but the ability to modulate their intensity and expression. They experience emotions more intensely, express them more impulsively, and have more difficulty calming down once aroused. Rating scales, direct observation, and physiological studies all converge on this finding 20.
Emotional dysregulation in ADHD does not only involve difficult emotions. It is better understood as emotional intensity in both directions. People with ADHD often experience low frustration tolerance, quick and disproportionate anger, difficulty self-soothing, and emotional reactivity that can look like mood instability. Yet the same nervous system that amplifies negative feelings also amplifies positive ones. Joy, passion, excitement, affection, and intimacy can be felt with unusual depth. Moments of connection can be profoundly moving, and even small experiences can evoke strong emotional responses, including tears, delight, or an almost overwhelming sense of closeness. Early in relationships, this can be misinterpreted as “love-bombing”, but it is usually not manipulative or strategic. It is the genuine, unfiltered expression of a nervous system that experiences emotions vividly and has limited braking capacity.
This broader emotional profile has significant implications for relationships. A partner who feels everything strongly, and who struggles to regulate the rise and fall of those feelings, may be more reactive during conflict, more affected by perceived rejection, and more changeable in their emotional state. Attempts to intervene through generic anger-management or communication-skills training often produce little visible improvement, because the underlying difficulty is not primarily with anger or communication. It is the untreated emotional dysregulation of ADHD, which is rooted in delayed development of the neural circuits responsible for impulse control and emotional self-regulation. Yet the same person may also bring warmth, enthusiasm, loyalty, and deep emotional engagement that can be uniquely enriching to a relationship. Recognising that this heightened emotionality is neurological rather than deliberate does not excuse harmful behaviour, but it does create a more compassionate framework for addressing it. Support only becomes effective when the ADHD itself is addressed.
We will return to emotional dysregulation in greater depth in Chapter 11, including practical strategies for both partners. For now, the key point is this: if you or your partner has ADHD and feels emotions intensely - whether painful or joyful - this is likely part of the condition, not a separate problem. It deserves the same thoughtful understanding and structured support as the attention and hyperactivity symptoms.
Time Blindness, Memory Irregularities, and Interest-Based Motivation
Ask someone with ADHD when something happened, and you may hear answers that are wildly out of sync with the actual timeline. A conversation that took place last week might feel as though it happened years ago, and a friend they “met years ago” may in fact have entered their life last month. This is not simply forgetfulness. It is a disturbance in the internal sense of time passing, often called time blindness, intertwined with differences in how memories are encoded, stored, and retrieved. Rather than experiencing time as a steady, continuous flow, many people with ADHD perceive it in irregular bursts, shaped by emotional intensity, levels of stimulation, and the inconsistent formation of memory. This makes the passage of time feel unpredictable and unreliable, and it is one of the most practically disruptive aspects of ADHD - yet one of the least understood by those who do not experience it.
Time blindness is not simply poor time management. It is a genuine perceptual difference in how the passage of time is experienced. Research has consistently demonstrated that people with ADHD show deficits in time perception and time estimation tasks 2122. They overestimate how much time has passed during short intervals and underestimate how much time tasks will take. An hour can feel like fifteen minutes when engaged in something interesting, or like an eternity when bored.
The Memory Connection
Memory and time perception are deeply interconnected. We construct our sense of “how long ago” something happened largely through memory - the clarity of a memory, its emotional weight, and how it connects to other memories all influence our perception of when it occurred. For people with ADHD, differences in how memories are formed and accessed create a chronological fog that compounds time blindness.
Working memory - the ability to hold information actively in mind while using it - is one of the executive functions most affected by ADHD 2324. This is the system that allows you to remember what you went upstairs to fetch, to hold the beginning of a sentence in mind while formulating the end, or to keep track of multiple steps in a task. When working memory is unreliable, information slips away before it can be consolidated into longer-term storage. The result is not that memories are gone, but that they were never properly filed in the first place.
Long-term memory in ADHD presents a different pattern. Many people with ADHD describe having excellent memory for certain things - song lyrics, facts about special interests, emotionally charged events - while having almost no recall for others, such as conversations, commitments, or routine daily events. This inconsistency reflects how the ADHD brain encodes information: experiences that generate sufficient dopamine activation (through novelty, emotional intensity, or personal interest) are remembered well, while experiences that do not reach that activation threshold may barely register at all.
Retrieval presents yet another challenge. Even when memories have been properly stored, accessing them on demand can be difficult. You may have had the experience of being unable to recall something in the moment, only to have it surface unbidden hours or days later - in the shower, while driving, in the middle of the night. This retrieval delay is common in ADHD. The memory exists; the pathway to access it is simply not available when needed. For partners, this can be maddening. “How can you not remember? We talked about this yesterday!” But for the person with ADHD, the memory may genuinely be inaccessible in that moment, only to return with perfect clarity at some random future point when it is no longer useful.
This memory profile has profound implications for relationships. Forgotten conversations, missed commitments, and inconsistent recall of shared experiences can feel like evidence that your partner does not care, does not listen, or does not value what matters to you. Understanding that this reflects neurological differences in memory encoding and retrieval - not a lack of love or attention - does not solve the practical problems, but it can prevent them from being interpreted as personal betrayal.
The Impact of Time Blindness
The practical implications of time blindness are enormous. People with ADHD chronically underestimate how long it takes to get ready, to complete tasks, to travel somewhere. They genuinely intend to be on time but consistently miscalculate. They start projects believing they have plenty of time, only to discover with shock that a deadline is tomorrow. They promise to “just finish this one thing” and emerge hours later, having missed appointments, meals, or important commitments.
Time blindness also produces a lesser-known but equally disruptive pattern: the complete reservation of attention for an upcoming event. Someone with ADHD who has an important appointment at 2pm may find themselves unable to do anything productive all morning. They know from experience that they cannot trust their internal sense of time. They know they are capable of becoming absorbed in a task and emerging hours later having missed the appointment entirely. So they compensate - by essentially putting their entire day on hold, mentally circling the upcoming event, unwilling to engage with anything else for fear of losing track of time. The morning is not spent relaxing; it is spent in a state of anxious vigilance, watching the clock, unable to settle. To a partner, this can look like laziness or poor planning. “You have five hours before you need to leave - why aren’t you doing anything?” But for the person with ADHD, those five hours feel like a minefield. They have learned that engaging with any task risks losing the appointment altogether, so they sacrifice the entire morning to ensure they do not miss it. This is time blindness turned inward - a compensatory strategy that works but at enormous cost to productivity and peace of mind.
This example illustrates something crucial that partners must understand: navigating ADHD in a relationship is not simply a matter of learning to accommodate the traits themselves. It also means navigating the layers of compensatory behaviours, coping mechanisms, and survival strategies that years of undiagnosed, unsupported ADHD have created. The person with ADHD has not been passively experiencing their condition - they have been actively adapting to it, often without understanding what they were adapting to. Some of these adaptations are ingenious. Others are maladaptive, born of desperation rather than insight. Many come with costs that are invisible until you live with someone closely enough to see the full picture. A partner is not just learning to live with ADHD; they are learning to live with the entire scaffolding of behaviours that a person built, often unconsciously, to survive in a world that was not designed for their brain.
Without reliable memory markers to anchor events in time, the past becomes a jumbled landscape where “recent” and “ages ago” lose their meaning. Did that argument happen last month or last year? Was it before or after the holiday? The emotional intensity of the memory may be vivid, but its location in time is vague. This can create friction in relationships when partners have very different recollections of when things occurred - not because anyone is lying, but because their brains are constructing timelines from different raw materials.
For partners, time blindness can feel like being deprioritised. When your partner is consistently late, consistently underestimates how long things take, consistently loses track of time while you wait - it can feel like they do not care about you or your time. Understanding time blindness as a perceptual and memory-based difference rather than a values statement does not eliminate the practical problems, but it can reduce the resentment and moral judgment that compound them.
The Interest-Based Nervous System
Closely related to time blindness and memory differences is what Dr William Dodson has called the “interest-based nervous system.” Neurotypical brains are largely “importance-based” - they can generate motivation based on the recognition that something is important, even if it is not interesting. ADHD brains struggle with this. They are “interest-based” - motivation comes relatively easily for things that are novel, interesting, challenging, or urgent, but is extremely difficult to generate for things that are routine, boring, or important but not immediately pressing.
This interest-based activation also shapes memory. Events, information, and experiences that engage the interest-based system are encoded strongly - sometimes with remarkable detail and permanence. Those that do not engage it may pass through awareness without leaving a trace. This is why someone with ADHD might remember an obscure fact from a documentary watched five years ago but have no recollection of a conversation about household finances from last Tuesday. The documentary activated their interest-based system; the finances conversation did not.
This explains some of the most frustrating paradoxes of ADHD. The same person who cannot motivate themselves to spend fifteen minutes on essential but boring paperwork can spend eight hours mastering a new skill that caught their attention. The same person who forgets routine appointments will move mountains when a crisis creates urgency. It is not that they do not understand what is important. It is that understanding something is important is not sufficient to generate the neurological activation needed to act on it - or to remember it.
The ADHD brain essentially has two time zones: “now” and “not now.” Things that are not immediately present, immediately urgent, or immediately interesting exist in a vague “not now” that has little motivational pull - and that may not be encoded into memory with any reliability. This is why artificial urgency (leaving things to the last minute) and external accountability (body doubling, working alongside others) can be so helpful - they create the “now” conditions that activate the ADHD brain and support both action and memory formation.
Tonic and Phasic States: The Dopamine Tide
Understanding ADHD requires understanding that the brain does not operate at a constant level of activation. Dopamine signalling happens in two modes: tonic (baseline, resting state) and phasic (stimulus-driven, task-engaged state). The interaction between these two modes helps explain many ADHD experiences.
Tonic dopamine refers to the baseline level of dopamine activity when you are not engaged in any particular task - your resting state of alertness and readiness. Phasic dopamine refers to the bursts of dopamine that occur in response to stimuli, rewards, or engaging tasks. In a well-functioning system, tonic levels provide stable baseline activation while phasic responses allow for sharpened attention and motivation when needed.
In ADHD, there appears to be dysregulation in this system. Research suggests that ADHD brains may exist in a state of chronic tonic underarousal - the baseline is set too low 25. This low baseline affects far more than motivation. It can influence working memory, executive control, emotional regulation, and even basic perceptual processes such as visual stability and sensory filtering. When tonic dopamine is too low, the world can feel slightly dimmed, inconsistent, or difficult to stay anchored to. Many ADHD individuals report a sense of “brain fog”. This creates a constant, subtle state of understimulation that drives much of what we observe in ADHD behaviour. The restlessness, the sensation-seeking, the difficulty tolerating boredom, the gravitating toward high-stimulation activities. These behaviours are not choices, but subconscious attempts to raise tonic activation to a functional level.
When phasic activation does occur - when something interesting, novel, or urgent captures attention - the ADHD brain may suddenly appear focused and capable. This is sometimes described as hyperfocus, but in many cases, the individual is not operating above their abilities; rather, they are finally operating at a normal functional level because phasic activation temporarily compensates for the low tonic baseline. The problem is that phasic activation is inconsistent and not under reliable voluntary control. It is stimulus-dependent, not effort-dependent.
This tonic/phasic framework has important implications for understanding daily functioning. The person with ADHD is not choosing to be unmotivated for boring tasks while energised for interesting ones. Their brain is providing inconsistent neurochemical support depending on stimulation levels. Tasks with low stimulation never receive adequate phasic activation, and the chronically low tonic baseline leaves the person feeling flat, foggy, or unable to initiate action. I explore this concept in much greater depth in Chapter 8, including how tonic underarousal can mimic depression and lead to misdiagnosis.
For relationships, understanding the tonic–phasic dynamic can be transformative. It helps explain why a partner with ADHD may seem like two different people: engaged, present, and capable during activities that provide adequate stimulation, even when the source of that stimulation is not obvious to anyone else, and then scattered, forgetful, or apparently unmotivated during routine daily life. For the partner, this pattern can feel confusing or even inconsistent, yet both states are genuine expressions of the same brain operating under different neurochemical conditions.
Common Comorbidities
ADHD rarely travels alone. Research consistently shows that the majority of people with ADHD have at least one additional mental health condition, and many have several. Dr Russell Barkley’s research suggests that more than 80% of adults with ADHD have at least one comorbid condition, more than 50% have two or more, and more than a third have three or more 20. Understanding these common companions to ADHD is essential for comprehensive treatment and for making sense of complex presentations.
Anxiety
Anxiety affects between 24% and 50% of adults with ADHD 2, making it one of the most common comorbidities - and one of the most commonly misunderstood.
For many people, anxiety is the presenting complaint that first brings them to a clinician’s attention. The racing thoughts, difficulty concentrating, restlessness, and sense of being overwhelmed can look very much like generalised anxiety disorder - and frequently, that is the diagnosis they receive, while the underlying ADHD goes unrecognised. We explore this diagnostic confusion in detail in Chapter 8.
Even when ADHD is correctly identified, anxiety frequently develops as a secondary condition - a learned response to decades of unpredictable difficulties, accumulated criticism, and the exhausting experience of knowing you are capable yet consistently underperforming. There is also growing evidence that ADHD and anxiety share neurobiological and genetic roots, which may explain why treating ADHD sometimes reduces anxiety that was downstream of dopamine dysregulation 2627. We examine the relationship between ADHD and secondary conditions more fully in Chapter 6.
Depression
Depression has a lifetime occurrence of around 53% in people with ADHD - far higher than the general population 28. Again, this makes sense. Years of struggling, underperforming relative to one’s potential, receiving negative feedback, and not understanding why everything is so hard takes a psychological toll. There is also evidence for shared neurobiological vulnerabilities. This connection also helps explain a common ADHD paradox: procrastination even on tasks the person genuinely wants to complete. For many people with ADHD, the anticipation of finishing something carries an unspoken dread - the knowledge that completion brings a crash, a return to understimulation, a depressive flatness that follows the loss of engaging focus. The task itself may not be the problem; the emptiness waiting on the other side of it is. Critically, Chapter 8 will discuss how ADHD-related dopamine dysregulation can create symptoms that look like depression but respond differently to treatment - what some call “dopamine starvation” or false depression.
Sleep disorders
Sleep disorders affect up to 70–78% of people with ADHD 29. Research has found that people with ADHD are significantly more likely to have delayed circadian rhythms - their biological clocks run late, making them prone to sleep-onset insomnia. In addition, many experience cognitive hyperarousal at bedtime: a racing or restless mind that does not “switch off,” making it difficult to wind down even when they feel physically tired 30629. The melatonin rise that triggers sleepiness occurs nearly two hours later in people with ADHD compared to controls. This creates a vicious cycle: poor sleep worsens ADHD symptoms, and ADHD-related difficulties winding down worsen sleep. Some researchers suggest that ADHD and sleep disorders may be bilateral comorbidities - conditions that share underlying causes and exacerbate each other.
Oppositional Defiant Disorder
ODD is present in 24–35% of people with ADHD and is particularly relevant for understanding conflict patterns. ODD involves patterns of angry, defiant, and vindictive behaviour. Barkley’s research suggests ODD has two components: an emotional component (anger, hostility, temper) that is often a direct expression of ADHD-related emotional dysregulation, and a social conflict component (defiance, resistance to authority) that is more environmentally shaped 6.
Addiction
Substance use disorders occur at elevated rates, with ADHD individuals showing higher rates of nicotine use, alcohol problems, and other substance misuse. Some of this represents self-medication - nicotine, for example, has stimulant properties and can temporarily improve ADHD symptoms. Understanding this does not excuse substance abuse but does suggest that treating the underlying ADHD is an important component of addressing substance problems.
The practical implication is that if you or your partner has ADHD and is also dealing with anxiety, depression, sleep problems, or other conditions, this is entirely typical. Treatment may need to address multiple conditions simultaneously, and what looks like one problem may actually be several interacting conditions. This is explored further in Chapter 7 and 8.
Diagnosis Across Demographics
ADHD does not discriminate by demographics, but diagnosis certainly has. Historically, ADHD was identified predominantly in young boys showing obvious hyperactive behaviour. This created a diagnostic prototype that has led to systematic under-identification of ADHD in anyone who does not fit that mould - particularly adults, those presenting with predominantly inattentive symptoms, and anyone who has learned to mask their difficulties.
The research on this point is clear: the fundamental nature of ADHD is the same regardless of sex, age, or background. Dr Barkley’s extensive research on sex differences in adult ADHD concludes that ADHD is “virtually the same in both sexes” - the core symptoms, underlying neurobiology, and executive function deficits are equivalent. The differences that do exist are small and largely reflect normal population differences rather than anything unique to ADHD 23.
Why, then, do diagnosis rates vary so dramatically? Several factors contribute. First, the diagnostic criteria were developed based primarily on research with hyperactive boys, so they capture that presentation most reliably. Second, hyperactive behaviour in childhood is disruptive and prompts referral, while inattentive symptoms are internal and easily overlooked. Third, there are different social expectations and tolerance for behaviour across different demographics - what is identified as problematic in one person may be overlooked or explained away in another.
The childhood ratio of approximately 3:1 in favour of diagnosis in boys declines substantially by adulthood, approaching 1.5:1 or even 1:1 in community samples 23. This suggests not that ADHD is more common in boys but that it is more likely to be identified in them. By adulthood, when hyperactivity has diminished and executive function deficits become more apparent across all affected individuals, the diagnostic gap narrows.
These diagnostic patterns of the past were not accidental. Historically, different behaviours were encouraged or discouraged along gendered lines in general. Boys were often permitted, even expected, to be physically active, noisy, or adventurous, while girls were discouraged from the same behaviours and rewarded for compliance. Because these underlying behavioural differences existed in the general population, early ADHD research simply reproduced them. More boys were identified with hyperactive ADHD not because the condition was more common in boys, but because the diagnostic lens was built on baseline behavioural norms rather than on the underlying neurobiology. In effect, early studies were sampling behaviour shaped by culture, not behaviour shaped by ADHD.
Modern social media has recreated this problem in a more insidious way. Posts titled “10 signs you have ADHD as a woman” imply that the condition manifests differently across sexes, despite evidence showing that ADHD has the same core neurobiology regardless of gender. These lists are not shaped by clinical insight but by engagement algorithms and audience-targeting strategies. Their purpose is to attract specific demographics, not to improve diagnostic accuracy, and in doing so they risk repeating the historical mistake of confusing culturally shaped expectations with the actual presentation of ADHD. If a man experiences the symptoms described in these lists, he still has ADHD. The condition does not participate in gender narratives, and framing it as though it does obscures recognition and leads to misdiagnosis. These narratives should be challenged rather than repeated, because they prioritise viewership over understanding and contribute to the very diagnostic distortions we are trying to correct.
What does this mean practically? If you are reading this book and recognise yourself or your partner in these descriptions but there is no formal diagnosis, that does not mean ADHD is not present. Many adults with ADHD have compensated, masked, or been overlooked for decades. The condition was there all along, shaping their lives in ways that may only become clear in retrospect. Late diagnosis is discussed extensively in Chapter 5.
The take-home message is this: ADHD is ADHD, regardless of who has it. The underlying neurology, the core symptoms, and the effective treatments are fundamentally the same. Demographic differences in diagnosis rates reflect biases in recognition and referral, not differences in the condition itself. If the symptoms fit and the impairment is present, the possibility of ADHD deserves investigation - regardless of whether someone “looks like” the stereotypical ADHD patient.
⁂
Pontifex, M. B., Saliba, B. J., Raine, L. B., Picchietti, D. L., & Hillman, C. H. (2013). Exercise Improves Behavioral, Neurocognitive, and Scholastic Performance in Children with Attention-Deficit/Hyperactivity Disorder. The Journal of Pediatrics, 162(3), 543–551. DOI: 10.1016/j.jpeds.2012.08.036 ↩
Key, A. P., & D’Ambrose Slaboch, K. (2021). Speech Processing in Autism Spectrum Disorder: An Integrative Review of Auditory Neurophysiology Findings. J Speech Lang Hear Res, 64(11), 4192–4212. DOI: 10.1044/2021_JSLHR-20-00738 ↩ ↩2
Antshel, K. M., & Russo, N. (2019). Autism Spectrum Disorders and ADHD: Overlapping Phenomenology, Diagnostic Issues, and Treatment Considerations. Current Psychiatry Reports, 21(5), 34. DOI: 10.1007/s11920-019-1020-5 ↩
Antshel, K. M., Zhang-James, Y., Wagner, K. E., Ledesma, A., & Faraone, S. V. (2016). An update on the comorbidity of ADHD and ASD: a focus on clinical management. Expert Review of Neurotherapeutics, 16(3), 279–293. DOI: 10.1586/14737175.2016.1146591 ↩
Sinclair, J. (1999). Why I dislike “person-first” language. ↩
Barkley, R. A. (2014). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment (Fourth ed.). Guilford Publications. [ISBN: 9781462538874]. ↩ ↩2 ↩3 ↩4
Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry, 171(3), 276–293. DOI: 10.1176/appi.ajp.2013.13070966 ↩ ↩2
Berridge, K. C., & Robinson, T. E. (1998). What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Brain Res Rev, 28(3), 309–369. DOI: 10.1016/s0165-0173(98)00019-8 ↩ ↩2
Wilens, T. E., & Morrison, N. R. (2011). The intersection of attention-deficit/hyperactivity disorder and substance abuse: . Current Opinion in Psychiatry, 24(4), 280–285. DOI: 10.1097/YCO.0b013e328345c956 ↩
Krause, K. H., Dresel, S. H., Krause, J., la Fougere, C., & Ackenheil, M. (2003). The dopamine transporter and neuroimaging in attention deficit hyperactivity disorder. Neurosci Biobehav Rev, 27(7), 605–613. DOI: 10.1016/j.neubiorev.2003.08.012 ↩
Faraone, S. V., & Larsson, H. (2019). Genetics of attention deficit hyperactivity disorder. Mol Psychiatry, 24(4), 562–575. DOI: 10.1038/s41380-018-0070-0 ↩
Figure 1: Schematic representation of dopamine biosynthesis, neurotransmission, and degradation. The diagram shows how dopamine (DA) is synthesised from tyrosine, packaged into vesicles, released into the synaptic cleft, and either broken down or recycled via the dopamine transporter (DAT). Adapted from Juza et al. (2023) 11. ↩
Figure 2: Distribution of the four major dopaminergic pathways in the human brain: nigrostriatal (SN), mesolimbic (NAc), mesocortical (VTA), and tuberoinfundibular (HN). These pathways govern movement, reward, cognition, and hormonal regulation respectively. Adapted from Juza et al. (2023) 11. ↩
Lee, J. S., Kim, B. N., Kang, E., Lee, D. S., Kim, Y. K., Chung, J. K., Lee, M. C., & Cho, S. C. (2005). Regional cerebral blood flow in children with attention deficit hyperactivity disorder: comparison before and after methylphenidate treatment. Hum Brain Mapp, 24(3), 157–164. DOI: 10.1002/hbm.20067 ↩
Rubinstein, J. S., Meyer, D. E., & Evans, J. E. (2001). Executive control of cognitive processes in task switching. J Exp Psychol Hum Percept Perform, 27(4), 763–797. DOI: 10.1037//0096-1523.27.4.763 ↩
Toplak, M. E., Rucklidge, J. J., Hetherington, R., John, S. C., & Tannock, R. (2003). Time perception deficits in attention-deficit/ hyperactivity disorder and comorbid reading difficulties in child and adolescent samples. J Child Psychol Psychiatry, 44(6), 888–903. DOI: 10.1111/1469-7610.00173 ↩
Juza, R., Musilek, K., Mezeiova, E., Soukup, O., & Korabecny, J. (2023). Recent advances in dopamine D2 receptor ligands in the treatment of neuropsychiatric disorders. Medicinal research reviews, 43(1), 55–211. DOI: 10.1002/med.21923 ↩
Figure 3: SPECT brain imaging comparing ADHD to healthy controls. Yellow arrows indicate areas of hypoperfusion (reduced blood flow/activity) in the orbitofrontal cortices. The ADHD brain shows significantly lower activity in prefrontal regions during both rest and concentration tasks. Adapted from Amen et al. (2021) 17. ↩
Kringelbach, M. L., & Berridge, K. C. (2017). The Affective Core of Emotion: Linking Pleasure, Subjective Well-Being, and Optimal Metastability in the Brain. Emotion Review, 9(3), 191–199. DOI: 10.1177/1754073916684558 ↩
Barkley, R. A. (2015). Research Findings. The ADHD Report, 23(4), 10–12. DOI: 10.1521/adhd.2015.23.4.10 ↩ ↩2
Smith, A., Taylor, E., Rogers, J. W., Newman, S., & Rubia, K. (2002). Evidence for a pure time perception deficit in children with ADHD. J Child Psychol Psychiatry, 43(4), 529–542. DOI: 10.1111/1469-7610.00043 ↩
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65. ↩
Castellanos, F. X., & Tannock, R. (2002). Neuroscience of attention-deficit/hyperactivity disorder: the search for endophenotypes. Nature Reviews Neuroscience, 3(8), 617–628. DOI: 10.1038/nrn896 ↩ ↩2 ↩3
Fu, X., Wu, W., Wu, Y., Liu, X., Liang, W., Wu, R., & Li, Y. (2025). Adult ADHD and comorbid anxiety and depressive disorders: a review of etiology and treatment. Front Psychiatry, 16, 1597559. DOI: 10.3389/fpsyt.2025.1597559 ↩
Shah, A., & Frith, U. (1983). An islet of ability in autistic children: a research note. J Child Psychol Psychiatry, 24(4), 613–620. DOI: 10.1111/j.1469-7610.1983.tb00137.x ↩
Ohi, K., Otowa, T., Shimada, M., Sasaki, T., & Tanii, H. (2020). Shared genetic etiology between anxiety disorders and psychiatric and related intermediate phenotypes. Psychological Medicine, 50(4), 692–704. DOI: 10.1017/S003329171900059X ↩
Van Veen, M. M., Kooij, J. J. S., Boonstra, A. M., Gordijn, M. C. M., & Van Someren, E. J. W. (2010). Delayed Circadian Rhythm in Adults with Attention-Deficit/Hyperactivity Disorder and Chronic Sleep-Onset Insomnia. Biological Psychiatry, 67(11), 1091–1096. DOI: https://doi.org/10.1016/j.biopsych.2009.12.032 ↩
Kaye, H. S., Jans, L. H., & Jones, E. C. (2011). Why Don’t Employers Hire and Retain Workers with Disabilities? Journal of Occupational Rehabilitation, 21(4), 526–536. DOI: 10.1007/s10926-011-9302-8 ↩
Matson, J. L., & Shoemaker, M. (2009). Intellectual disability and its relationship to autism spectrum disorders. Research in developmental disabilities, 30(6), 1107–1114. DOI: https://doi.org/10.1016/j.ridd.2009.06.003 ↩ ↩2
Barratt, A., Bell, K., Thomas, R., McGeechan, K., & Kazda, L. (2019). Evidence of Potential Overdiagnosis and Overtreatment of ADHD in Children and Adolescents: Protocol for a Scoping Review. BMJ Open. DOI: 10.1136/bmjopen-2019-032327 ↩